Old Drugs That Are Still Good Drugs
Carol Peckham; Mary L. Windle, PharmD; Ashley Kenkel, PharmD
October 18, 2013
The Classics — the 1800s
- Aspirin. Derived from willow bark, aspirin has been marketed since 1899. Today, aspirin is an essential part of many treatment regimens for cardiovascular disease, including myocardial infarction (MI) prevention, initial MI treatment (chewable aspirin), and MI/stroke recurrence prevention.
- Morphine. Derived from opium, morphine was first sold in 1827. Since then, morphine has been formulated as various delivery methods, including oral, rectal, IV, transdermal, and extended-release formulations such as liposomal injection and oral products for chronic pain control, including patient-controlled analgesia. Opioid analgesics that have physical properties that deter abuse (eg, injecting dissolved oral tablets) have been approved.
- Insulin. Insulin was identified in 1869 and was first used in humans in the 1920s. Since its discovery, many formulations have been developed, including short-acting (aspart, lispro), long-acting (detemir, glargine), and combinations. Other routes, such as the recently approved inhaled insulin, allow additional options.
Image courtesy of Wikimedia
The Classics — the 1900s
• Penicillin. Penicillin was discovered in 1928 when Alexander Fleming observed that colonies of Staphylococcus aureus could be destroyed by penicillin mold. Use as an antibiotic began in the 1940s. Today it still has activity against many microbes and is commonly used for the treatment of streptococcal infections. The general class includes cephalosporins and carbapenems.
• Corticosteroids. In the 1930s, six hormones were isolated from adrenal glands. Cortisone was first used in 1948 to treat a patient with rheumatoid arthritis.[1] Today corticosteroids are available in many formulations and are the mainstay of treatment for chronic illnesses, such as inflammatory bowel disease and asthma. New drug delivery systems, such as intravitreal inserts for macular edema, provide small amounts of drug delivered to a precise location and last for several years.
• Isoniazid. Isoniazid was first synthesized in 1912, and activity against tuberculosis was identified in 1945. More than 100 years later, isoniazid is still a standard treatment of TB, by itself for latent infection and in combination for treatment of active disease.
Image from Thinkstock

Nitroglycerin
Nitroglycerin (NG) was first used by William Murrell to treat anginal attack. The discovery was published in 1878, but it was not until 2002 that the enzyme, mitochondrial aldehyde dehydrogenase, was discovered to convert NG to the potent vasodilator nitric oxide.[2] It is still recommended in major guidelines for immediate relief of angina.[3] Researchers continue to find new uses and new forms. For example, NG has been found to reduce bone resorption and improve bone formation[4,5] and is being studied for possible use in healing diabetes-induced foot ulcers.[6] The nitrate-nitrite-nitric oxide pathway was investigated as a therapeutic approach to metastatic prostate cancer.[7,8] Of interest, the New York Times reported in 2010[9,10] that 80% of the almost 5 million prescriptions for sublingual NG tablets were unapproved because of FDA regulations that did not require approval for drugs marketed before 1938. Today there are multiple routes of administration, including oral, IV, sublingual, topical, and rectal. NG rectal administration was recently approved for anal fissure pain relief, via nitric oxide's effect on internal anal sphincter relaxation.
Image from Medscape
Colchicine
Use of colchicine, a compound in the autumn crocus (Colchicum autumnale), dates as far back as 1500 BC, and its first recorded treatment for gout was in the first century AD. Colchicine had been available generically after being grandfathered in by the FDA, which did not require approval for drugs marketed before 1938. In 2009, however, the FDA granted URL Pharma an exclusive license, and its branded version, Colcrys, increased in price from 10¢ to $5 a pill.[11] The drug can have serious adverse effects, notably from interaction with clarithromycin, but it's still an important treatment for gout and familial Mediterranean fever and is also beneficial for treating recurrent aphthous ulcers.[12] In addition, colchicine's antimitotic activity is being investigated for use in cancer therapy,[13-15] and its neutrophilic properties are being explored for cardiovascular protection.[16] A recent study reported benefit in treating endocarditis.[17]
Image courtesy of Wikimedia

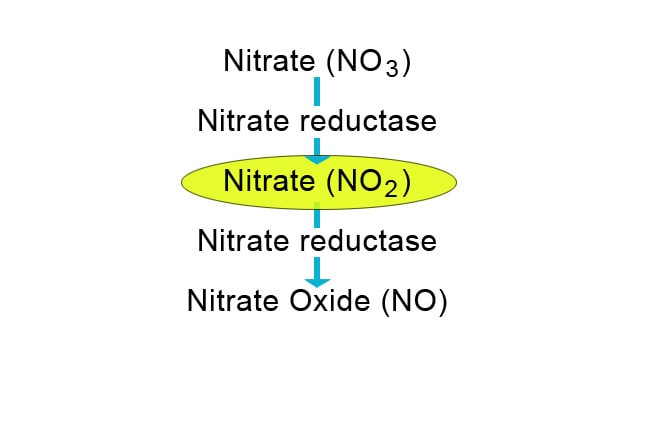
Thiazide Diuretics
Early diuretics were herbal derivatives, in use at least since the 16th century when they were key agents for treating edema, called "dropsy." The first diuretic compounds were organomercurials, which were replaced by carbonic anhydrase in the mid-1940s. By 1960, the thiazide hydrochlorothiazide and thiazide-like chlorthalidone had been approved, and as early as 1959, the American Heart Association and the National Institutes of Health reported declining death rates, which they partly attributed to the new thiazide antihypertensives.[18] Their value in treating hypertension has remained steady. Although superiority of chlorthalidone over hydrochlorothiazide has been proven for the most part, some debate remains.[19] Thiazide diuretics are often recommended as first-line therapy for the treatment of hypertension when no other comorbidities exist.
Image from Medscape
Spironolactone
Spironolactone, a weak diuretic and aldosterone antagonist, was introduced clinically in 1959. It has long been useful as an add-on drug in treating high blood pressure and is proving to be effective in some patients with resistant hypertension.[20] It is important in the treatment of patients with heart failure,[21-23] and recent guidelines now recommend it for NYHA Class II-IV patients.[24,25] As a diuretic, spironolactone is often used in combination with furosemide for the treatment of edema/ascites caused by liver cirrhosis. Its potent antiandrogen properties have also made it a useful agent in treating male pattern baldness and hirsutism, alopecia, and acne in females. Spironolactone is now proving to be effective when added to metformin to treat polycystic ovaries.[26,27] Eplerenone, a newer aldosterone antagonist, along with other new structurally related agents, may eventually supersede spironolactone.[28] No head-to-head studies have been conducted to date, however, and spironolactone is inexpensive, so it is still the standard in this class.
Image courtesy of Wikimedia
Monoamine Oxidase Inhibitors: Rescuing the Neurorescuers
MAOIs, powerful antidepressant and antianxiety agents in use for over 50 years, act on serotonin, norepinephrine, and dopamine receptors. After initial popularity, their use dropped dramatically with the introduction of SSRIs along with perhaps exaggerated concerns about drug/food interactions (eg, "cheese reaction").[29,30] Interest in MAOIs was renewed after studies reported significant adverse effects with SSRIs and newer antidepressants, including difficulty attaining remission.[31] The availability of a MAOI-B transdermal formulation (selegiline), which limits the need for dietary restrictions and has fewer sexual and metabolic effects than newer antidepressants, has also helped.[32,33] Transdermal delivery allows much lower dosing by avoiding first-pass metabolism in the gut (where orally ingested MAOIs knock out the metabolism of dietary tyramine as it is absorbed, the mechanism leading to hypertensive effects). But this does not eliminate the potential for serotonin crises if combined with other antidepressants. MAOI-B's have also shown neuroprotective and neurorescue properties[34] and have been proven beneficial in other conditions, including Parkinson disease.[35,36]
Image from Thinkstock

Warfarin
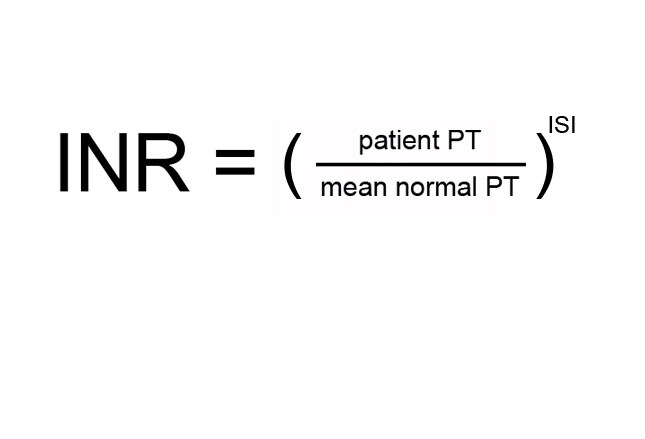
Warfarin's effects were first noted in the 1920s when cattle that ate spoiled sweet clover died of hemorrhagic disease. The anticoagulant compound causing the bleeding, dicoumarol, was not identified until the 1940s. Warfarin in a more potent form was introduced in 1948 as a rodenticide and is still used for this purpose. In 1954, it was approved for prevention of thrombosis and thromboembolism and is still the most widely prescribed oral anticoagulant in North America. The need for regular INR monitoring has always been a shortcoming, resulting in lower adherence.[37] Newer oral anticoagulants include the direct thrombin inhibitor dabigatran, and Factor Xa inhibitors rivaroxaban and apixaban, which do not require INR monitoring and in some studies show an edge over warfarin.[38,39] However, warfarin's low cost and the ability to rapidly reverse bleeding still put it in the lead. An antidote for Factor Xa inhibitors is currently undergoing phase 3 clinical trials.[40] Fresh frozen plasma and prothrombin complex concentrate are being investigated, although their onset of action is not prompt. There is also indication evidence that the newer agents may pose a higher risk for GI bleeding.[41,42]
Image from Medscape
Metformin
First synthesized in the 1920s, metformin was neglected for the next 2 decades as research focused on insulin and other antidiabetes drugs. The 1940s saw resurging interest in metformin's ability to reduce blood glucose, and in 1957 it was first tested for diabetes. It wasn't introduced to the United States, however, until 1995. Metformin is the only drug that has conclusively been shown to prevent the cardiovascular complications of diabetes,[43,44] and there are some reports that it might reduce the risk for cancers.[45-47] It is currently (in the absence of contraindications) recommended by the AACE/ACE, ADA/EASD, and ACP as the first-line oral therapy for type 2 diabetes.[48] It has been combined with other antidiabetes medications, such as glipizide and sitagliptin, in single-pill formulations. As of 2010, metformin and glibenclamide are the only 2 oral antidiabetes agents in the World Health Organization Model Lists of Essential Medicines. Metformin has also become an important agent in treating polycystic ovary syndrome and its complications.[49,50]
Images from Wikimedia; First Data Bank

The Tetracyclines
The tetracyclines were discovered as natural products in 1945 and were first prescribed in 1948. Chlortetracycline (Aureomycin®) was the first of these agents and was derived from Streptomyces aureofaciens, a golden-colored, fungus-like, soil-dwelling bacterium. In the 1950s, a research team determined the chemical structure and fermentation process for tetracycline, which was then patented in 1955. Within 3 years, it was the most prescribed broad-spectrum antibiotic in the United States.[51] Tetracyclines are used for urinary tract infections, chlamydia, spirochetal infections, anthrax, plague, tularemia, and Legionnaires disease. Minocycline and doxycycline are also used for the treatment of acne. Recent research is focusing on their anti-inflammatory properties,[52] particularly the potential for neuroprotection against Alzheimer disease, stroke, Parkinson disease, and AIDS-related dementia.[53-57]
Image courtesy of Wikimedia
